
Contents
Concise Communication
Impact of antimicrobial use in dogs on antimicrobial resistance and shared flora with human owners
-
- Published online by Cambridge University Press:
- 09 January 2023, e1
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antibiotic Stewardship
SG-APSIC1059: Impact of a single intervention as part of a antimicrobial stewardship in a surgical unit of a tertiary-care referral center for neurosurgery
-
- Published online by Cambridge University Press:
- 16 March 2023, p. s1
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Top Poster Award
Antibiotic Stewardship
Clinical factors and diagnoses associated with inappropriate urine-culture ordering in primary care
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s1
-
- Article
-
- You have access
- Open access
- Export citation
Letter to the Editor
Increase in the incidence of Candida parapsilosis and Candida tropicalis bloodstream infections during the coronavirus disease 2019 (COVID-19) pandemic
-
- Published online by Cambridge University Press:
- 10 January 2023, e2
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Poster Presentation - Top Poster Award
Antibiotic Stewardship
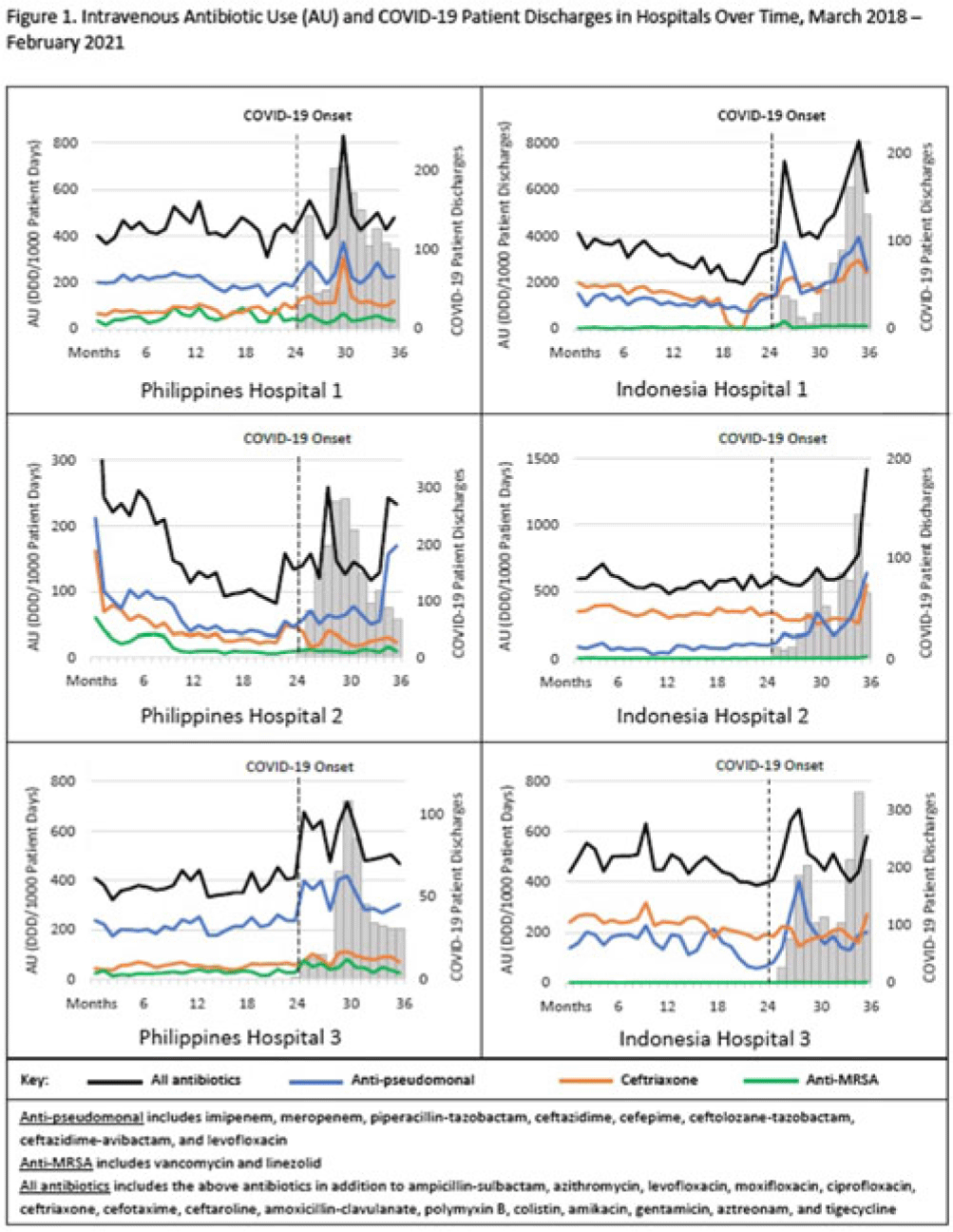
Impact of the COVID-19 pandemic on inpatient antibiotic use in Indonesia and the Philippines
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s1-s2
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The coronavirus disease 2019 (COVID-19) pandemic severely affected Southeast Asia, with >35 million cases and ~360,000 deaths. Despite relatively low rates of secondary bacterial infection among inpatients with COVID-19, several countries reported increased antibiotic use; raising concerns for worsening antimicrobial resistance. We assessed the impact of the COVID-19 pandemic on the use of antibiotics commonly used to treat respiratory infections in Southeast Asia. Methods: We evaluated intravenous antibiotic use among hospitalized adults in acute-care wards in 6 hospitals; 3 in Indonesia and 3 in the Philippines. We abstracted data on antibiotics that are commonly used to treat respiratory infections in these hospitals. We calculated antibiotic use rates for the 25 included antibiotics as monthly defined daily dose per 1,000 patient days (or patient discharges where patient days was unavailable) using data from pharmacy dispensing records and administrative records. Median antibiotic use rates for the prepandemic period (March 2018–February 2020) and the pandemic period (March 2020–February 2021) were compared, and percentage changes were calculated for (1) all 25 antibiotics combined; (2) ceftriaxone; (3) vancomycin and linezolid combined (anti-MRSA); and (4) broad-spectrum antibiotics with activity against Pseudomonas aeruginosa (anti-PSA). Monthly antibiotic use and COVID-19 patient discharges were graphed over the 36-month study period (March 2018–February 2021) to visualize trends (Fig. 1). The Wilcoxon rank-sum test was used to determine whether differences in median antibiotic use rates were statistically significant (2-tailed P < .05). Results: Overall, trends in antibiotic use were higher during months with increased COVID-19 patient discharges (Fig. 1). Use of all 25 antibiotics combined significantly increased in 4 of 6 hospitals (6.9%–63.6%) during the pandemic period compared to the prepandemic period. Ceftriaxone use significantly increased in 3 of 6 hospitals (37.1%–55.4%) and decreased in 3 of 6 hospitals (15.9%–31.9%). Anti-PSA antibiotic use significantly increased in 4 of 6 hospitals (16.1%–161.5%). Although anti-MRSA antibiotic use was low (comprising <2% of the overall included antibiotic use in Indonesia and <11% in the Philippines), use during the pandemic increased in 3 of 6 hospitals (59.8%–212.6%). Conclusions: We observed substantial increases in antibiotic use among hospitalized adults in Indonesia and the Philippines during the COVID-19 pandemic. The increased use of broad-spectrum antibiotics is concerning given the potential consequence of worsening antimicrobial resistance. Understanding how increases in antibiotic use compares to rates of bacterial infection, antimicrobial resistance, and antibiotic availability and accessibility during this time is important to contextualize results. These findings reinforce the importance of antibiotic stewardship practices to optimize antibiotic use, especially during pandemics.
Disclosure: None

Antibiotic Stewardship
SG-APSIC1093: Engaging inpatients in antibiotic stewardship efforts: The need to enhance knowledge and increase involvement in their antibiotic therapy
-
- Published online by Cambridge University Press:
- 16 March 2023, p. s1
-
- Article
-
- You have access
- Open access
- Export citation
Original Article
Going local: Evaluating guideline adherence and appropriateness of antibiotic prescribing in patients with febrile neutropenia at an academic teaching hospital
-
- Published online by Cambridge University Press:
- 09 January 2023, e3
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antibiotic Stewardship
SG-APSIC1101: Virulence factors and antimicrobial resistance in coagulase-negative staphylococci isolated from blood of neonates
-
- Published online by Cambridge University Press:
- 16 March 2023, pp. s1-s2
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Top Poster Award
Antibiotic Stewardship
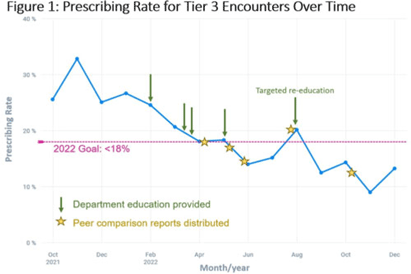
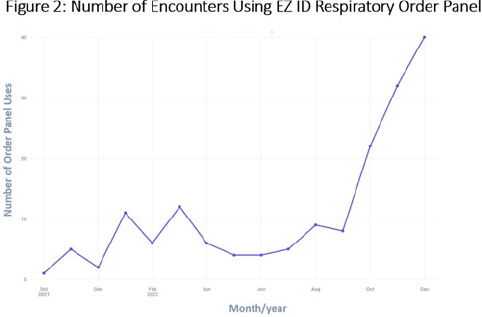
Multi-faceted approach to decreasing inappropriate antibiotic prescribing for viral upper respiratory tract infections
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s2
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Prescribing of antibiotics for viral upper respiratory infection (URI) remains a pressing public health problem. We sought to reduce inappropriate prescribing of antibiotics for viral URIs at primary-care practices at Mayo Clinic Arizona (MCA). Methods: Diagnostic codes for URIs commonly caused by viruses were categorized as tier 3 (ie, never prescribe). The inappropriate prescribing rate was defined as the number of tier 3 encounters resulting in a prescription for a URI antibiotic divided by the total number of tier 3 encounters. MCA primary-care departments, including family medicine, community internal medicine, emergency medicine, and women’s health internal medicine, were included in the intervention. Each department was briefed on the project, including baseline department prescribing data, and was provided education. Education topics included appropriate indications for antibiotics, patient-centered strategies for reducing antibiotic use, and a review of electronic resources developed specifically for the project. Resources included a syndromic ambulatory order panel (EZ ID Respiratory Order Panel) and a viral prescription pad, which contains simplified over-the-counter recommendations for symptomatic management of viral URIs and patient education. Quarterly peer comparison reports were provided to the department chairs and/or site leads. Our goal was to reduce inappropriate prescribing by 22% in 2022. An Epic dashboard (SlicerDicer model) was developed to track data on an ongoing basis. We used χ2 tests to compare categorical variables. Results: Department education was completed by June 2022 (Fig. 1). The annual antibiotic prescribing rate for tier 3 encounters decreased by 29% from a baseline rate 23.6% in 2021 to 16.4% in 2022 (P < .001). The posteducation prescribing rate (June 2022–December 2022) was 13.1%. Utilization of the EZ ID ambulatory order panel increased from an average of 1.5 uses per month in 2021 to 13.3 uses per month in 2022 (Fig. 2). Repeated healthcare contact for URIs within 14 days of tier 3 encounters did not differ among patients prescribed and not prescribed an antibiotic in all of 2022 (3.8% vs 3.9%; P = .91) or during the posteducation period (1.8% vs 4.2%; P = .14). There was no appreciable diagnostic shift over the course of 2022 (Fig. 3). Conclusions: A multifaceted intervention, which included baseline education, promotion of syndrome-specific order panels, dissemination of resources for symptomatic management, and distribution of peer comparison reports, resulted in significant reduction of inappropriate antibiotic prescribing for URIs.
Disclosure: None


Antibiotic Stewardship
SG-APSIC1074: Trend of ‘ESKAPE’ and their susceptibility changes for meropenem and levofloxacin during the pandemic at Sardjito Hospital Yogyakarta Indonesia
-
- Published online by Cambridge University Press:
- 16 March 2023, p. s2
-
- Article
-
- You have access
- Open access
- Export citation
Commentary
Bacteriuria in older adults triggers confusion in healthcare providers: A mindful pause to treat the worry
-
- Published online by Cambridge University Press:
- 09 January 2023, e4
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Poster Presentation - Top Poster Award
Antibiotic Stewardship
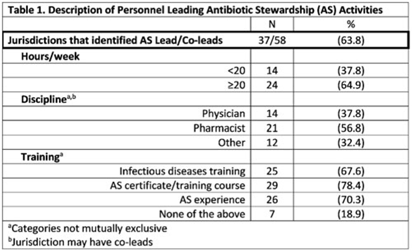
Description of antibiotic stewardship expertise and activities among US public health departments, 2022
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s3
-
- Article
-
- You have access
- Open access
- Export citation
-
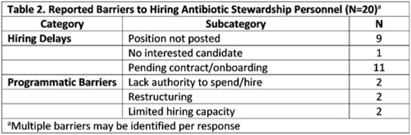
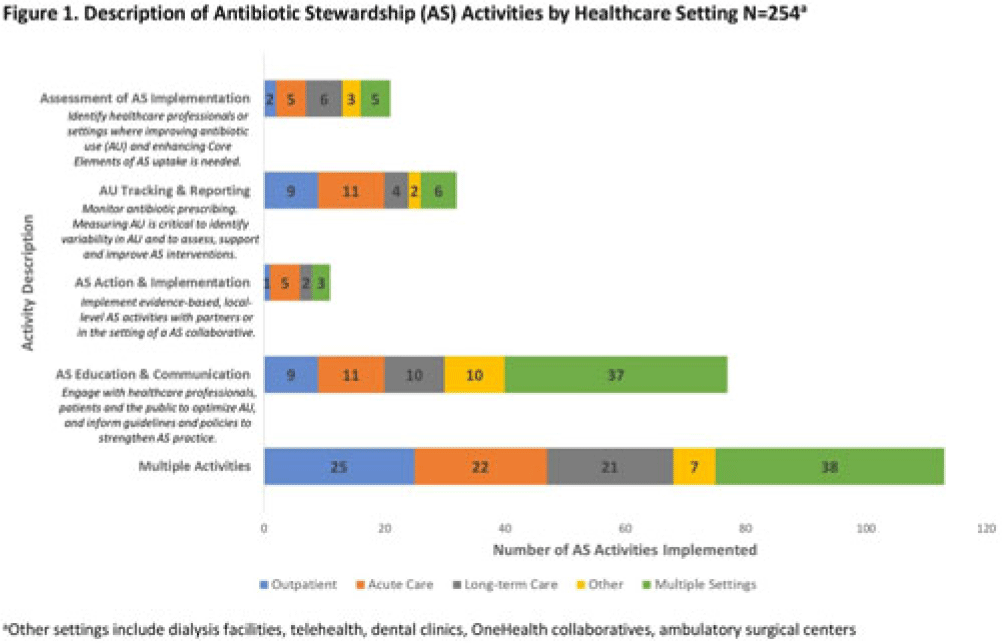
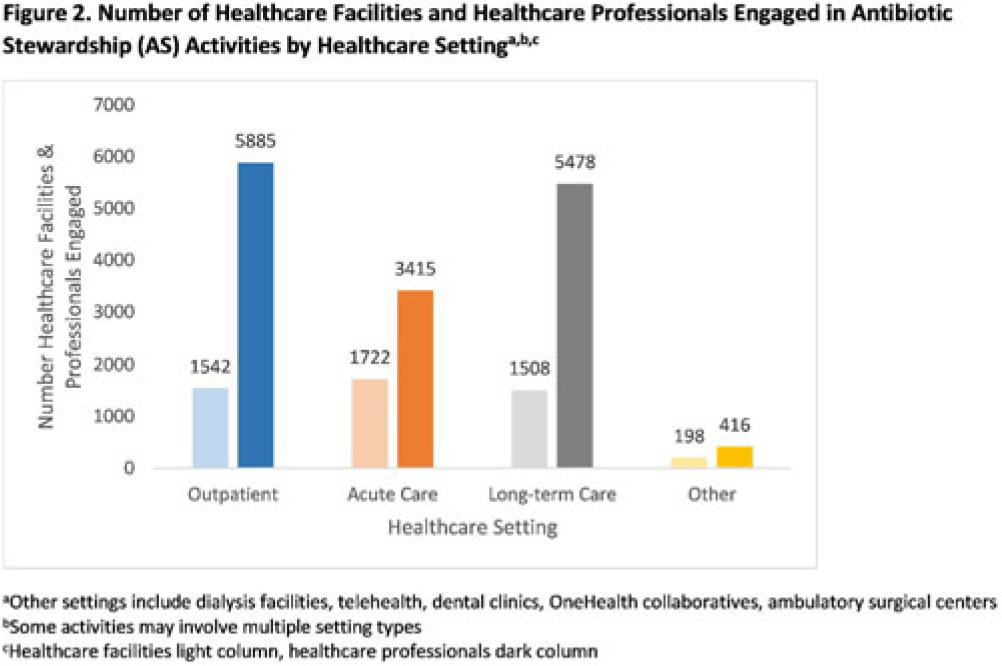
Background: In 2021, the CDC awarded >$100 million to 62 state, local, and territorial health departments (SLTHDs) to expand antibiotic stewardship expertise and implement antibiotic stewardship activities in different healthcare settings. Our objective was to describe SLTHD antibiotic stewardship personnel and activities to characterize the impact of the funding. Methods: SLTHDs submitted performance measures, including quantitative and qualitative responses, describing personnel supporting antibiotic stewardship activities, types of activities, and healthcare facilities and professionals engaged from January through June 2022. A quantitative analysis of performance measures and qualitative thematic analysis of select narrative responses are reported. Results: Most SLTHDs (58 of 62, 94%) submitted performance measures. Among them, 37 (64%) reported identifying an antibiotic stewardship leader or coleader; most were pharmacists (57%) or physicians (38%) with infectious diseases training (68%) (Table 1). Of the remaining STLHDs, 20 reported barriers to identifying a leader or coleader, including hiring process delays and programmatic barriers (Table 2). SLTHDs reported 254 antibiotic stewardship activities; most reported activities involving multiple activity types (44%). Education and communication (eg, providing stewardship expertise) was the most common single activity (30%), followed by antibiotic use tracking and reporting (13%), assessment of antibiotic stewardship implementation (8%), and action and implementation (eg, audit and feedback letters) (4%). The highest number of activities were implemented in multiple healthcare settings (35%), followed by acute care (21%), outpatient (18%), long-term care (17%), and other (9%) (Fig. 1). SLTHDs reported engaging 4,970 healthcare facilities and 15,194 healthcare professionals in antibiotic stewardship activities across healthcare settings, to date, as part of this funding opportunity (Fig. 2). Conclusions: Antibiotic stewardship funding to SLTHDs allowed for increases in capacity and expanded outreach to implement a variety of antibiotic stewardship activities across multiple healthcare settings. Sustaining STLHD antibiotic stewardship activities can help increase engagement and coordination with healthcare facilities, healthcare professionals, and other partners to optimize antibiotic prescribing and patient safety.
Disclosure: None




Fear of missing organisms (FOMO): Diabetic foot and osteomyelitis management opportunities
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s3-s4
-
- Article
-
- You have access
- Open access
- Export citation
-
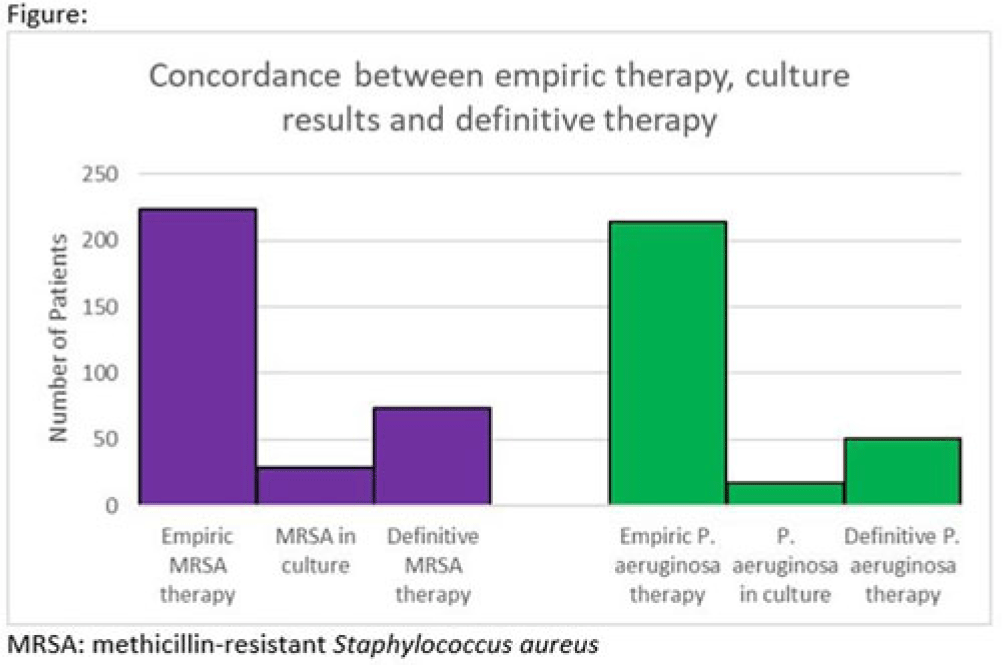
Background: Hospitalizations for diabetic foot infections and lower-extremity osteomyelitis are common. Use of empiric antibiotic therapy for methicillin-resistant Staphylococcus aureus (MRSA) and Pseudomonas aeruginosa is also common. Guidelines recommend antibiotic therapy based on severity of illness, risk factors for MRSA and P. aeruginosa, and local prevalence. We evaluated the concordance between empiric antibiotic therapy and both culture results and definitive antibiotic therapy with a focus on MRSA and P. aeruginosa. We also evaluated how well MRSA and pseudomonal risk factors were predictive of culture results with these organisms. Methods: We conducted a cohort study of all patients admitted to our hospital system in 2021 with a diagnosis of a diabetic foot infection or lower-extremity osteomyelitis. Patients were included if they had an International Classification of Disease, Tenth Revision (ICD-10) diagnosis code of M86, E10.621, E11.621, or E08.621. Patients were excluded if antibiotics were for another indication or if they were aged <18 years. In patients with multiple hospitalizations only the first hospitalization was included. Empiric antibiotic therapy included antibiotics started by the admitting team. Definitive antibiotic therapy included the final antibiotic course either completed during admission or prescribed at the time of discharge. MRSA risk factors included prior positive culture with MRSA within the last year, hospitalization with IV antibiotics within 90 days, intravenous drug use, or hemodialysis. Pseudomonal risk factors included prior positive culture with P. aeruginosa within the last year or hospitalization with IV antibiotics within 90 days. Results: In 2021, 260 unique patients were admitted with suspected diabetic foot infections or lower-extremity osteomyelitis. 68 patients had >1 admission. Empiric anti-MRSA and antipseudomonal therapy was administered to 224 (86%) and 214 (82%) patients, respectively. Definitive anti-MRSA and antipseudomonal therapy was administered to 76 (30%) and 51 (20%) patients, respectively. Of the 195 patients who had wound cultures, 29 (15%) and 18 (9%) had positive cultures for MRSA and P. aeruginosa respectively (Fig.). The negative predictive value of MRSA risk factors for predicting a negative culture with MRSA was 91%. The negative predictive value of pseudomonal risk factors for predicting a negative culture with P. aeruginosa was 95%. Conclusions: Our data suggest an opportunity for substantial reductions in empiric anti-MRSA and antipseudomonal therapy for diabetic foot infection and lower-extremity osteomyelitis. The absence of MRSA and pseudomonal risk factors was reasonably good at predicting the absence of a positive culture with these organisms.
Disclosure: None

Original Article
Clinical impact of a multiplex rapid diagnostic pneumonia panel in critically ill patients
-
- Published online by Cambridge University Press:
- 09 January 2023, e5
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
COVID-19
SG-APSIC1208: Association between severity of COVID-19 pneumonia and vaccination status in a tertiary-care teaching hospital in Malaysia
-
- Published online by Cambridge University Press:
- 16 March 2023, p. s2
-
- Article
-
- You have access
- Open access
- Export citation
Original Article
Multinational prospective cohort study of rates and risk factors for ventilator-associated pneumonia over 24 years in 42 countries of Asia, Africa, Eastern Europe, Latin America, and the Middle East: Findings of the International Nosocomial Infection Control Consortium (INICC)
-
- Published online by Cambridge University Press:
- 09 January 2023, e6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
COVID-19
SG-APSIC1053: Detection of SARS-COV-2 in nasopharyngeal swags with MALDI-TOF MS and machine learning
-
- Published online by Cambridge University Press:
- 16 March 2023, pp. s2-s3
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Top Poster Award
Antibiotic Stewardship
Inpatient pediatric antimicrobial use for respiratory infections during the RSV surge
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s4-s5
-
- Article
-
- You have access
- Open access
- Export citation
-
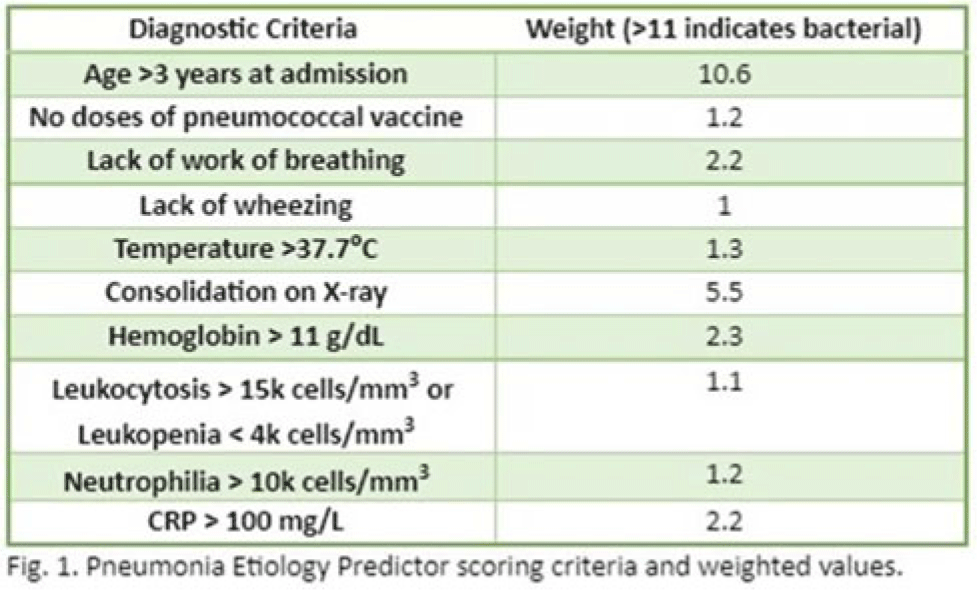
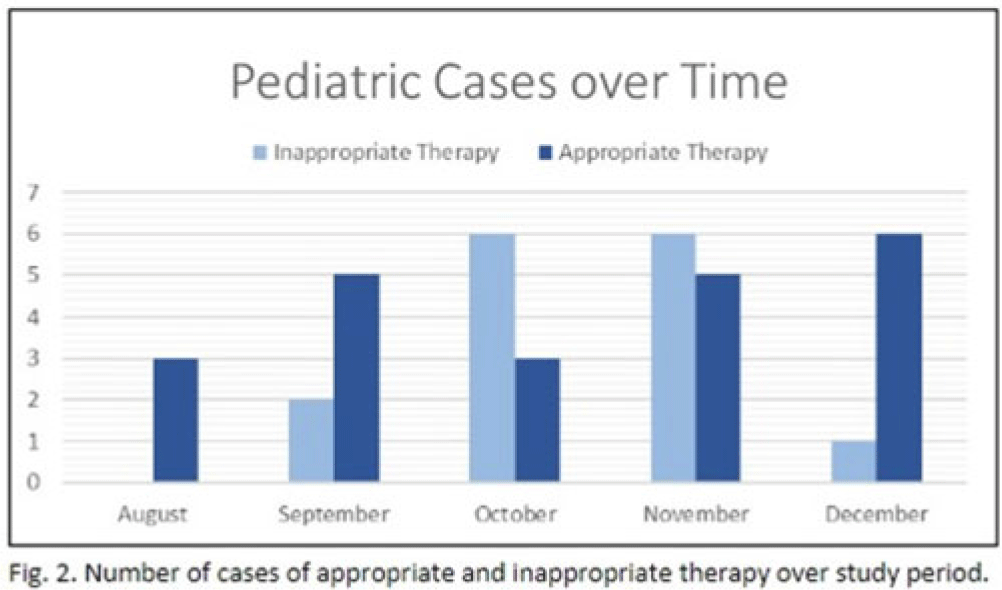
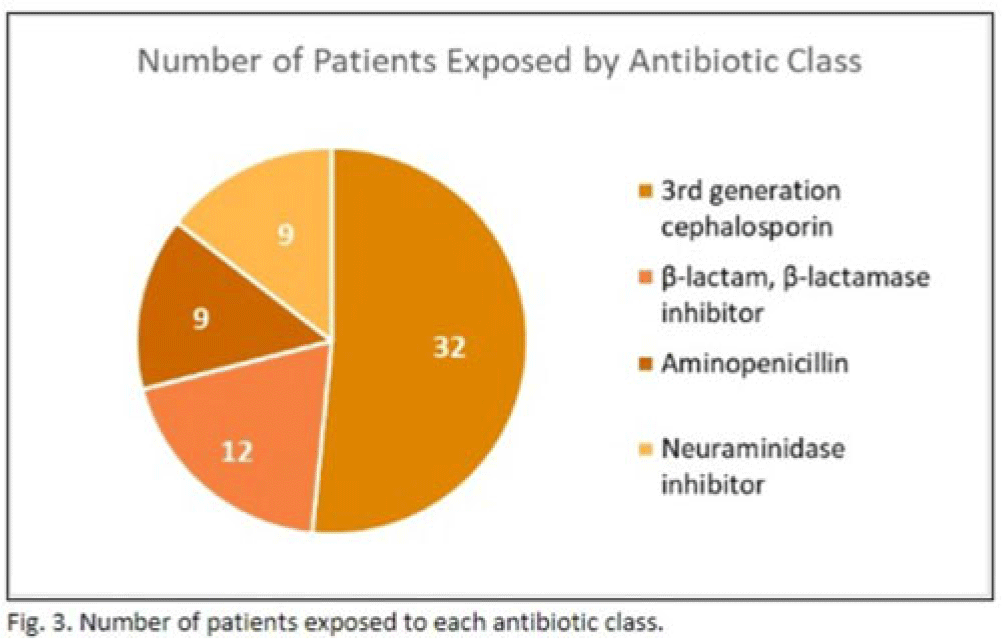
Background: In the United States, pneumonia causes >100,000 pediatric hospitalizations annually. On November 4, 2022, the CDC issued a Heath Advisory concerning an upcoming surge of respiratory illnesses including SARS-CoV-2, influenza, and respiratory syncytial virus (RSV). Differentiating between viral and bacterial causes is challenging and can lead to antimicrobial overuse. Currently, tools are being developed to distinguish between viral and bacterial pneumonia. The VALS-DANCE Pneumonia Etiology Predictor (PEP) provides clinical scoring criteria (Fig. 1) to determine probable cause of pneumonia with 93.1% sensitivity for bacterial pneumonia. Scores >11 have a >25% likelihood of having bacterial etiology. Given that antimicrobial exposure increases resistance rates, disrupts natural flora, and increases the risk of side effects, a core goal of researchers is to develop ways to promote stewardship and reduce inappropriate use. We assessed the patterns of use for antimicrobials in pediatric patients admitted with pneumonia at our institution. Methods: This retrospective review included pediatric cases admitted to an urban safety-net community hospital from July 22, 2022, to December 16, 2022. A daily list of all patients receiving antimicrobials was reviewed, and pediatric patients with diagnosis of a respiratory infection were included. Patients with additional indications for antimicrobial therapy, diagnosis of bronchitis, incomplete records, or without complete information were excluded from the scoring criteria. The primary objective was to assess the appropriateness of antimicrobial use for pneumonia, defined as use consistent with PEP scoring recommendations. Results: Of 53 patients reviewed, 37 met inclusion criteria. Of 37 patients, 22 (59.5%) met study criteria for appropriate therapy. The 15 patients (40.5%) who were inappropriate for treatment received an average of 4.67 ± 1.91 days of antibiotics. Of these 15 patients, 11 (73.3%) also had a positive viral test, further increasing the likelihood of a viral etiology. This subgroup had an average antibiotic exposure of 4.27 ± 1.79 days. Documented rationale for therapy included severity of illness (4 of 11), radiograph consolidation (4 of 11), and provider disagreement with radiograph interpretation (3 of 11). Conclusions: Pediatric respiratory infections represent a significant opportunity for antimicrobial stewardship. In this study, as many as 40% of pediatric patients may have received unnecessary antibiotic exposure. Use of the VALS-DANCE criteria may help clinicians identify patients with low likelihood of bacterial infection and reduce antimicrobial use. The national surge of viral infections serves to highlight the vital importance of appropriate diagnostic stewardship.
Disclosure: None



Research Brief
Detection of SARS-CoV-2 from combined nasal/rectal swabs
-
- Published online by Cambridge University Press:
- 09 January 2023, e7
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Poster Presentation - Top Poster Award
C. difficile
Integrated efficacy analysis from phase 3 studies of investigational microbiome therapeutic, SER-109, in recurrent Clostridioides difficile infection
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s5
-
- Article
-
- You have access
- Open access
- Export citation
-
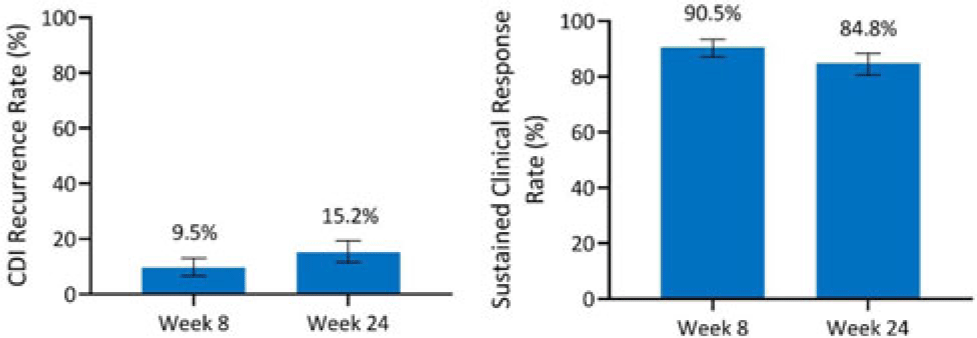
Background: Antibiotics alone are often insufficient to treat recurrent C. difficile infection (rCDI) because they have no activity against C. difficile spores that germinate within a disrupted microbiome. SER-109, an investigational, oral, microbiome therapeutic comprised of purified Firmicutes spores, was designed to reduce rCDI through microbiome repair. We report an integrated efficacy analysis through week 24 for SER-109 from phase 3 studies, ECOSPOR III and ECOSPOR IV. Methods: ECOSPOR III was a randomized, placebo-controlled phase 3 trial conducted at 56 US or Canadian sites that included 182 participants with ≥2 CDI recurrences, confirmed via toxin EIA testing. Participants were stratified by age (<65 years or ≥65 years) and antibiotic regimen (vancomycin, fidaxomicin) and were randomized 1:1 to placebo or SER-109 groups. ECOSPOR IV was an open-label, single-arm study conducted at 72 US or Canadian sites including 263 participants with rCDI enrolled in 2 cohorts: (1) rollover participants from ECOSPOR III who experienced on-study recurrence diagnosed by toxin EIA (n = 29) and (2) participants with ≥1 CDI recurrence (diagnosed by PCR or toxin EIA), inclusive of the current episode (n = 234). In both studies, the investigational product was administered orally as 4 capsules over 3 consecutive days following symptom resolution after standard-of-care antibiotics. The primary efficacy end point was rCDI (recurrent toxin-positive diarrhea requiring treatment) through week 8. Other end points included CDI recurrence rates and safety through 24 weeks. Results: These 349 participants received at least 1 dose of SER-109 in ECOSPOR III or ECOSPOR IV (mean age 64.2; 68.8% female). Overall, 77 participants (22.1%) enrolled with their first CDI recurrence. Four participants received blinded SER-109 in ECOSPOR III followed by a second dose of open-label SER-109 in ECOSPOR IV. Overall, the proportion of participants who received any dose of SER-109 with rCDI at week 8 was 9.5% (33 of 349; 95% CI, 6.6 %–13.0%), and the CDI recurrence rate remained low through 24 weeks (15.2%, 53 of 349; 95% CI, 11.6%–19.4%), corresponding to sustained clinical response rates of 90.5% (95% CI, 87.0%–93.4%) and 84.8% (95% CI, 80.6%–88.4%), respectively (Fig. 1). Most rollover participants (25 of 29, 86.2%) were from the placebo arm; 13.8% had rCDI by week 8. Conclusions: In this integrated analysis, the rates of rCDI were low and durable in participants who received the investigational microbiome therapeutic SER-109, with sustained clinical response rates of 90.5% and 84.8% at weeks 8 and 24, respectively. These data further support the potential benefit of microbiome repair with SER-109 following antibiotics for rCDI to prevent recurrence in high-risk patients.
Financial support: This study was funded by Seres Therapeutics.
Disclosure: None
